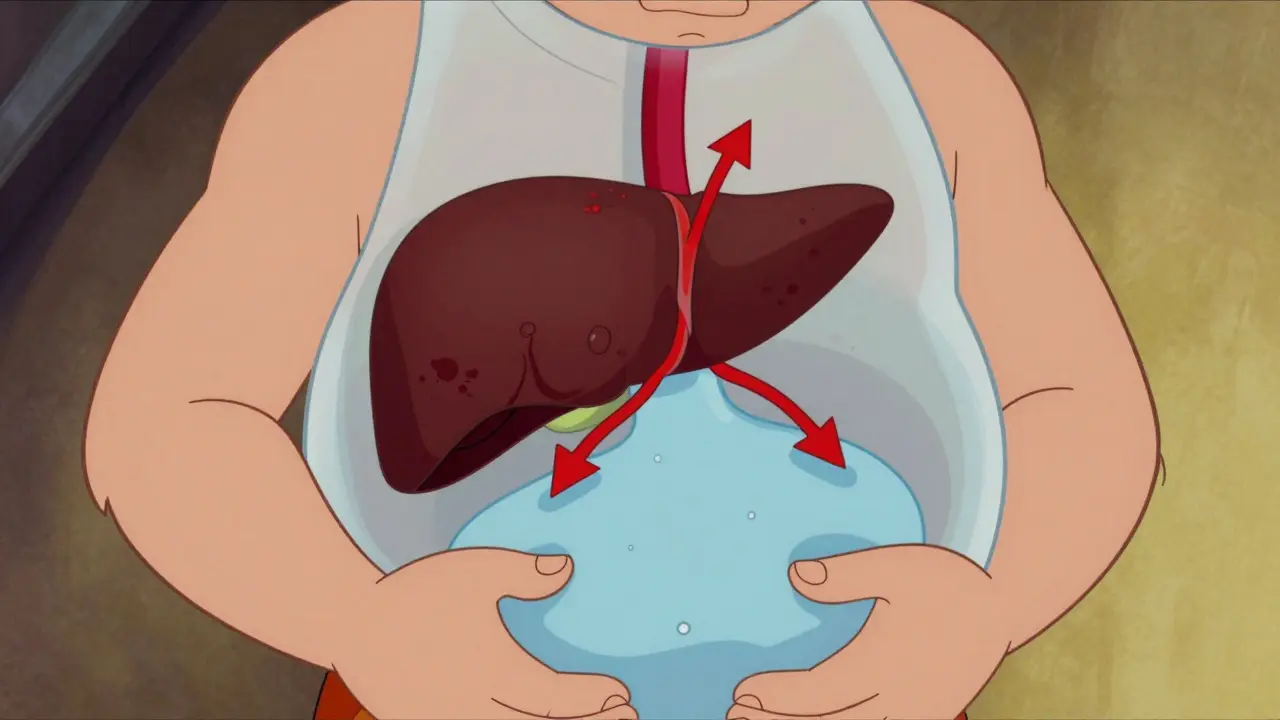
Fluid pooling in the abdomen is not just uncomfortable; it is a critical warning sign that your liver is struggling. This condition, known as ascites, which is the pathological accumulation of fluid in the peritoneal cavity, affects roughly half of all patients diagnosed with cirrhosis within ten years. For those facing this diagnosis, understanding how to manage fluid retention is often the difference between stability and hospitalization. The standard approach involves two main pillars: limiting salt intake and using specific medications called diuretics.
However, medical guidelines are currently shifting. While traditional advice demanded strict sodium limits, new research suggests this might sometimes do more harm than good. Navigating these conflicting signals can be overwhelming. Let’s break down exactly what the science says about managing ascites today, focusing on practical steps you can discuss with your hepatologist.
The Core Problem: Why Fluid Builds Up
To treat ascites effectively, you first need to understand why it happens. It isn't simply a matter of drinking too much water. The root cause lies in portal hypertension, which is increased blood pressure in the portal vein system. When scar tissue forms in the liver due to cirrhosis, blood flow is blocked. This causes pressure to build up behind the blockage, forcing fluid out of the blood vessels and into the abdominal cavity.
Simultaneously, your kidneys perceive this pressure change as low blood volume. In response, they hold onto every bit of sodium and water they can find. According to the European Association for the Study of the Liver (EASL), ascites develops when sodium excretion falls below dietary intake. If the pressure gradient across the liver exceeds 12 mmHg, fluid leakage becomes inevitable. This creates a vicious cycle: more fluid leads to higher pressure, which leads to even more fluid retention.
Sodium Restriction: The Traditional Standard vs. New Evidence
For decades, the rule was simple: cut the salt. The American Association for the Study of Liver Diseases (AASLD) has historically recommended restricting dietary sodium to less than 2 grams per day. To put that in perspective, 2 grams of sodium equals about 5 grams of table salt, or roughly one teaspoon. This amount covers everything you eat in a single day, including processed foods, restaurant meals, and snacks.
Why such a strict limit? The goal is to create a "negative sodium balance," where your body excretes more salt than it consumes. Since water follows salt, losing sodium helps pull fluid out of the abdomen. However, recent studies have challenged this dogma. A 2022 study published in the Gut and Liver Journal found that patients on unrestricted diets (5-6.5 grams of salt daily) actually resolved their ascites at higher rates (45%) compared to those on strict restrictions (16%).
This contradiction exists because extreme sodium restriction can reduce blood flow to the kidneys. In some cases, this triggers hepatorenal syndrome, which is a serious kidney complication associated with advanced liver disease, raising mortality risks. Dr. Pere Gines, a leading investigator in this field, argues that strict restriction may be counterproductive when combined with proper diuretic therapy. Many experts now advocate for a "moderate" approach, aiming for no more than 5-6.5 grams of salt daily, rather than the rigid 2-gram limit.

Diuretics: How They Work and Dosing Protocols
Diet alone rarely solves ascites. Most patients require medication to help the kidneys flush out excess fluid. These drugs are called diuretics, or "water pills." There are two primary types used in liver disease management:
- Spironolactone, which is a potassium-sparing diuretic that blocks aldosterone: This is usually the first line of defense. It works by blocking aldosterone, a hormone that tells your kidneys to retain salt. Starting doses typically range from 100 to 200 mg daily, increasing every 72 hours up to a maximum of 400 mg.
- Furosemide, which is a loop diuretic that acts on the kidney tubules: Often added if spironolactone isn’t enough. It starts at 40 mg daily and can go up to 160 mg. It works faster but can deplete potassium levels.
Doctors often prescribe these together in a 100:40 ratio (spironolactone:furosemide) to maintain electrolyte balance. The therapeutic goal is gradual weight loss: no more than 0.5 kg (1.1 lbs) per day if you don’t have leg swelling, or 1 kg (2.2 lbs) per day if you do. Losing weight too quickly can shock the kidneys and worsen liver function.
Monitoring and Safety: What to Watch For
Managing ascites requires close monitoring. You cannot guess whether the treatment is working; you must measure it. Here are the key metrics your healthcare team will track:
| Metric | Target / Warning Sign | Frequency |
|---|---|---|
| Weight Loss | <0.5 kg/day (no edema); <1 kg/day (with edema) | Daily |
| Serum Sodium | Avoid dropping below 130 mEq/L (hyponatremia risk) | Twice weekly during initiation |
| Kidney Function (Creatinine) | Stable or improving; sharp rise indicates stress | Weekly or as directed |
| Potassium Levels | Normal range; high risk with Spironolactone | Regularly during titration |
Hyponatremia (low blood sodium) occurs in 30-40% of ascites patients. If your sodium drops below 130 mEq/L, doctors may adjust diuretics or restrict free water intake. Never stop taking your medications without consulting your doctor, as sudden cessation can lead to rapid fluid re-accumulation.
When Diuretics Fail: Refractory Ascites
About 5-10% of patients develop refractory ascites, which is fluid buildup that does not respond to sodium restriction and diuretics. This is a serious development, associated with a 50% survival rate at six months if untreated. When diuretics max out or cause side effects like kidney failure, other interventions become necessary:
- Large-Volume Paracentesis: A needle is inserted into the abdomen to drain liters of fluid at once. This provides immediate relief but doesn't fix the underlying issue. Fluid often returns within days.
- Albumin Replacement: After draining large volumes, doctors infuse human albumin (8g per liter removed) to prevent circulatory dysfunction and kidney injury.
- TIPS Procedure: Transjugular Intrahepatic Portosystemic Shunt creates a bypass in the liver to lower portal pressure. It’s effective but carries risks of hepatic encephalopathy (brain fog).
- Vaptans: Vasopressin receptor antagonists help excrete water without losing salt. However, they are expensive ($5,000-$7,000 per course) and limited to short-term use.
Practical Tips for Daily Life
Living with ascites means making conscious choices about food and activity. Here is how to implement sodium management without feeling deprived:
- Read Labels Carefully: 75% of dietary sodium comes from processed foods, not the salt shaker. Avoid canned soups, deli meats, frozen dinners, and chips. Look for products labeled "low sodium" or "no salt added."
- Cook Fresh: Prepare meals at home using fresh herbs, spices, lemon juice, and garlic for flavor instead of salt.
- Watch Out for Hidden Sources: Baking soda, monosodium glutamate (MSG), and certain antacids contain hidden sodium.
- Avoid NSAIDs: Drugs like ibuprofen and naproxen can worsen kidney function and increase bleeding risk. Use acetaminophen cautiously and only under medical supervision.
- Protein Intake: Malnutrition affects 35-90% of cirrhotic patients. Do not starve yourself. Ensure adequate protein intake unless your doctor advises otherwise due to encephalopathy.
How much salt should I really eat if I have ascites?
Traditional guidelines recommend less than 2 grams of sodium (5 grams of salt) per day. However, recent evidence suggests a moderate restriction of 5-6.5 grams of salt daily may be safer and equally effective for many patients, especially when combined with diuretics. Always follow your hepatologist's specific advice, as individual kidney function varies.
Can I drink alcohol if I have ascites?
No. Alcohol accelerates liver damage and worsens portal hypertension. Complete abstinence is critical to preventing further decompensation and complications like spontaneous bacterial peritonitis.
What are the signs that my ascites is getting worse?
Warning signs include rapid weight gain (more than 2-3 pounds in a day), increased abdominal girth, shortness of breath, swelling in the legs or feet, and confusion or drowsiness. Contact your doctor immediately if you experience fever or abdominal pain, as these could indicate infection.
Why do I need to take both Spironolactone and Furosemide?
These drugs work on different parts of the kidney. Spironolactone blocks aldosterone to save potassium, while Furosemide forces rapid water and sodium excretion but loses potassium. Taking them together balances electrolyte levels while maximizing fluid removal.
Is paracentesis painful?
The procedure is generally well-tolerated. Doctors use local anesthesia to numb the skin, so you may feel pressure or a slight pinch, but sharp pain is uncommon. Relief from abdominal pressure is often felt immediately after drainage.
Madeline Petes
May 21, 2026 AT 19:15ok so i read this and my head is spinning but also kinda relieved. the part about not starving yourself on protein was huge for me because every time i go to the doctor they act like im gonna explode if i eat a chicken breast. its wild how much advice changes depending on who you ask. thanks for breaking down the salt thing though, i was literally measuring out teaspoons of salt with a ruler before reading this. feels like we are all just guessing until someone explains it clearly.
Jonhnnie john13
May 23, 2026 AT 01:19the study cited from gut and liver journal is flawed methodology. sample size too small and no control group for diuretic dosage variance. you cannot compare unrestricted diet patients to restricted ones without normalizing the spironolactone intake. typical cherry picking by researchers wanting to publish contrary findings. stick to the aasld guidelines or die faster.
Gary Helminiak
May 24, 2026 AT 05:43Hey there! 👋 I wanted to add a bit more context to what Jonhnnie mentioned regarding those studies. It is absolutely true that clinical trials in hepatology can be tricky to interpret because liver disease progresses at such different rates for different people. The key takeaway really isn't necessarily that you should ignore your doctor's orders on salt but rather that rigid adherence to a 2 gram limit might cause more harm than good if it leads to malnutrition or kidney stress. Many nephrologists now prefer looking at the overall sodium balance rather than just the input number. It is a nuanced field! 🌿
Elizabeth Fandry
May 25, 2026 AT 03:47One must consider the philosophical implications of bodily autonomy versus medical paternalism 🧐. When institutions dictate the precise milligram of sodium one may ingest they strip away the fundamental human experience of culinary choice. This is not merely about fluid retention; it is about the erosion of self. The pretension of believing that a teaspoon of salt holds the power of life and death is absurdly elitist. We are not vessels to be calibrated but beings to be lived. 😤
Ramanath Rao
May 26, 2026 AT 15:00Stop making excuses for bad science. In India we see thousands of cases where doctors prescribe whatever is easiest not what works. You think western medicine is perfect? Look at the cost of vaptans mentioned here $5000 per course. Who pays that? Poor people die while rich people buy their way out. The system is broken globally. Do not trust these guidelines blindly. They protect hospital revenue not patient lives.
Nivetha Narayanan
May 27, 2026 AT 23:14hey everyone! just wanted to say that even though this topic is super heavy i feel like sharing our stories helps so much. i have been dealing with ascites for two years now and honestly the worst part was feeling alone in it. knowing that others are navigating the same confusing advice about salt and meds makes me feel less crazy. lets keep supporting each other okay? 💖
Frank Arlyss
May 28, 2026 AT 14:02i dont care about your studies or your feelings. i am tired of seeing people complain about side effects when they could just accept the pain as part of living. stop seeking validation online and deal with your own bodies. nobody wants to hear about your weight loss goals or your electrolyte levels. it is boring and selfish.
irine sabrina
May 28, 2026 AT 16:54I completely understand why Frank feels that way sometimes the noise can be overwhelming but please know that your health journey is valid and important to share. It takes immense courage to discuss chronic conditions openly. I hope you find a community here that respects your boundaries while still offering the support you deserve. Your well-being matters deeply to many of us. ✨
Tim Reynolds
May 29, 2026 AT 03:28The FDA approved these drugs for profit. Not health. Spironolactone causes gynecomastia in men which is a known side effect often ignored. Big Pharma knows this. They want dependent patients. Do not take the pills. Drink water. Eat natural foods. The portal hypertension theory is a myth created to sell shunts. Wake up people. The truth is hidden in plain sight. ;)
Ryan Jones
May 30, 2026 AT 02:23everyone says follow the guidelines but the guidelines change every five years. first it was strict salt then moderate salt now maybe no restriction. why do we keep trusting them? probably because the doctors get paid to write the guidelines. i bet if they were poor they would suggest eating pickles and drinking beer. classic manipulation of the masses. sad really.
Lisa Russo
May 30, 2026 AT 06:51you guys are overthinking this. just eat less salt. if your belly gets big stop eating processed food. its not rocket science. why do we need complex charts and ratios? common sense works fine. stop blaming the government for your bad diet choices.
Sharon O’Mahonh
June 1, 2026 AT 02:22look i get that simple advice sounds nice but the physiology is actually quite complex. the renin-angiotensin-aldosterone system goes haywire in cirrhosis. its not just about eating salt its about how your body handles volume overload. ignoring the hormonal drivers is like trying to fix a computer by hitting it. we need to engage with the biochemistry not just throw around platitudes about common sense. let us dive deeper into the molecular mechanisms together.
Gareth Tyler
June 2, 2026 AT 06:25i guess the point is that every body is different. some people respond well to low salt others crash. i just weigh myself every morning and adjust based on the scale. if i gain more than a pound i cut back on dinner carbs. seems to work for me. no drama needed.
Groman Neta
June 2, 2026 AT 19:24This article is poorly written. It presents conflicting information without resolving the contradiction. Readers will leave confused. The author lacks editorial discipline. Furthermore the table formatting is amateurish. A professional publication would not publish such a mess. Disappointing effort.
Anthony Padilla
June 4, 2026 AT 17:42thanks for sharing this info everyone. i have a friend who is going through this and i want to help him cook better meals. does anyone have recipes that are low sodium but still taste good? i am trying to make something with herbs and lemon like the post suggested but i am not a great cook. any tips would be awesome!